These are relatively common fractures in elderly individuals as the spine is one of the first bones to lose bone density and the mechanics of the spine is such that the lack of bone strength can often result in spine fractures even with little to no injuries to the spine. Hence, even the simplest of manoeuvres to a weak spine such as bending forward to pick up weight (without an actual history of falls or trauma to the body) can leave the spine most vulnerable to osteoporotic stress fractures. Similarly, in the case of falls/ injuries, the loading weight on the spine in addition to the force of injury that the individual's spine is susceptible to can result in compression fractures.
Cause of injuries:
- Injuries to the spine such as fall in a sitting position, or high-velocity injuries such as road traffic accidents and fall from height injuries.
- In the cases of severely weakened bones. Bending forward for prolonged periods when the spinal bone (vertebra is too weak to handle such a manoeuvre)
Preferred treatment option:
The type of treatment mainly depends on factors such as:
- Spine fractures that also cause an injury to the spinal cord, which is enclosed within the vertebra, vary in severity, ranging from simple fractures to multiple fragment fractures.
- The threat of the current fracture to injure the enclosed spinal cord.
- Risk of spinal deformity if the fracture is untreated or inadequately treated.
Depending on these factors:
Non-operative management for simple wedge compression fractures which have retained significant height even after the compression and do not pose a threat to the spinal cord or risk of progressive spinal deformity.
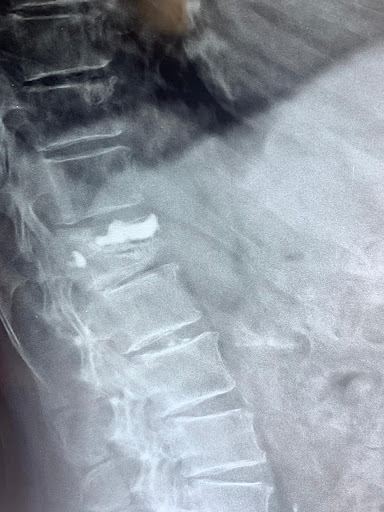
In case of stable spine fractures which pose no threat to the spinal cord but cause severe prolonged pain of the back, an alternative minimally invasive option of treatment involves a day care procedure known as Vertebroplasty or kyphoplasty under local Anaesthesia.
Surgical spinal stabilisation using rods and screws are reserved for “burst” fractures which are unstable, pose a risk of spinal cord injuries (or have already resulted in a spinal cord injury) or the the fractured vertebrae is too severely crushed to achieve any adequate restoration of the height of the vertebral body via minimally invasive procedures such as Vertebroplasty/ kyphoplasty.
Recovery Period:
In spine fractures where conservative or non operative modality of management is pursued, the individual will require a minimum of 4 weeks of STRICT bed rest following which the patient is then reassessed and started on walking exercises and other spinal rehabilitation activities.
In individuals who have undergone minimally invasive treatment (Vertebroplasty or kyphoplasty) the patient is mobilized immediately after the procedure (pain-free) and is allowed to walk with no restrictions. The patient is then allowed to resume all his/ her routine activities within 5 to 7 days.
In individuals upon whom spinal stabilization surgery is performed, the individual is allowed to get out of bed and start walking within 24 hours and can resume all activities within 2 weeks.